Fill Out a Valid New Mexico Report Template
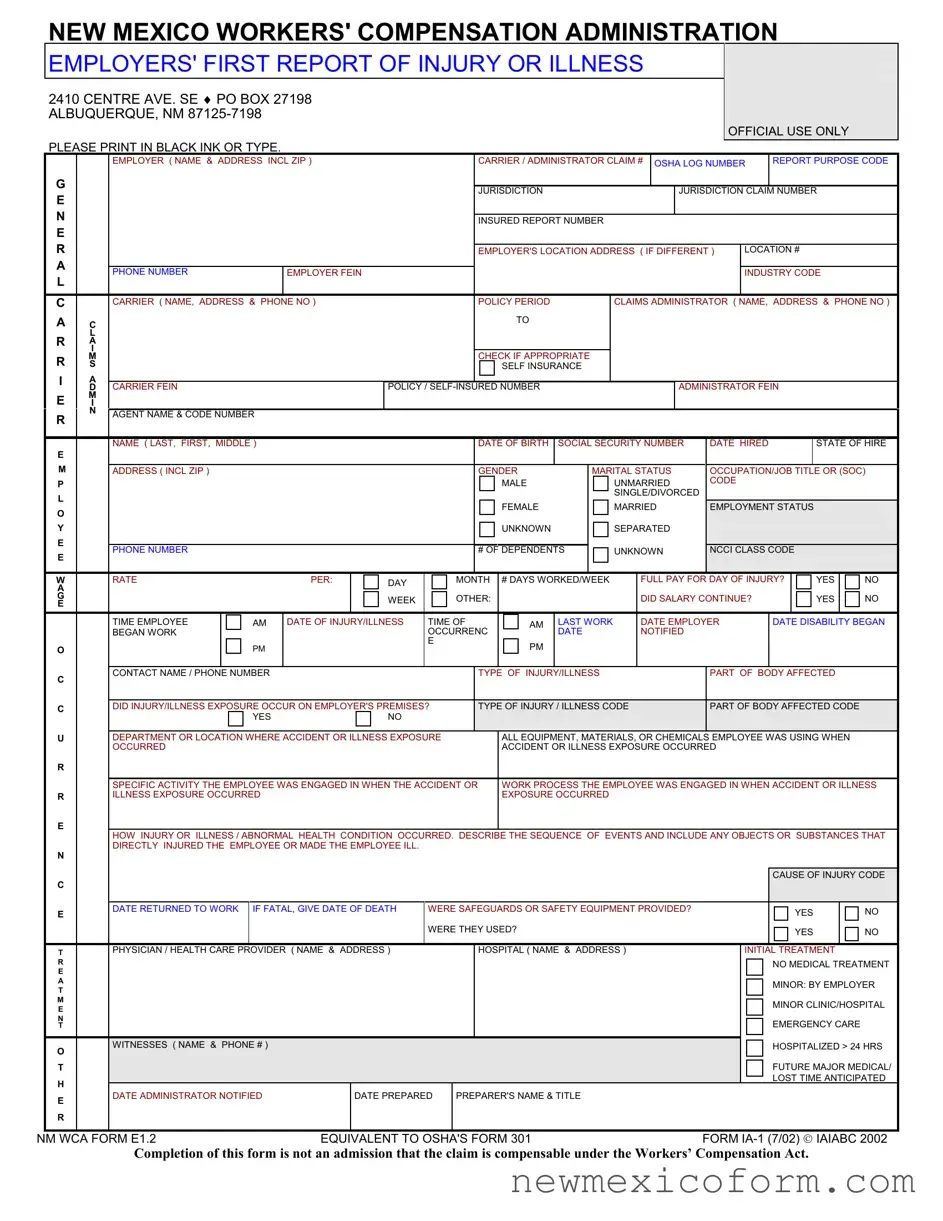
The New Mexico Workers' Compensation Administration requires the Employers' First Report of Injury or Illness to be diligently completed and submitted for any work-related injuries or illnesses that result in more than seven days of lost work or, unfortunately, in the death of a worker. Located in Albuquerque with multiple regional offices, the administration emphasizes the need for accurate and prompt reporting, ensuring that all involved parties—employers, insurance carriers, and the injured employees—are aware of and adhere to their responsibilities and rights under the Workers' Compensation Act. This form, filled out in black ink or typed, captures detailed information about the employee, the employer, the insurance carrier, and the specifics of the injury or illness, including the type, cause, and circumstances leading to it. Additionally, it asks for details on the initial treatment and any witnesses, while also indicating whether safety equipment was provided or used. Filing this report is crucial not just for compliance and potential fines avoidance but also for facilitating the proper processing of workers' compensation claims. It plays a vital role in ensuring that workers who are injured or fall ill on the job receive appropriate medical treatment and compensation for their injuries or illnesses, emphasizing the importance of workplace safety and the well-being of employees.
Document Preview
NEW MEXICO WORKERS' COMPENSATION ADMINISTRATION
EMPLOYERS' FIRST REPORT OF INJURY OR ILLNESS
2410 CENTRE AVE. SE ♦ PO BOX 27198 ALBUQUERQUE, NM
OFFICIAL USE ONLY
PLEASE PRINT IN BLACK INK OR TYPE.
EMPLOYER ( NAME & ADDRESS INCL ZIP ) |
CARRIER / ADMINISTRATOR CLAIM # OSHA LOG NUMBER |
REPORT PURPOSE CODE |
G |
|
|
|
|
|
|
|
|
E |
|
|
|
|
JURISDICTION |
|
JURISDICTION CLAIM NUMBER |
|
|
|
|
|
|
|
|
|
|
N |
|
|
|
|
|
|
|
|
|
|
|
|
INSURED REPORT NUMBER |
|
|
|
|
|
|
|
|
|
|
|
|
|
E |
|
|
|
|
|
|
|
|
R |
|
|
|
|
|
|
||
|
|
|
|
EMPLOYER'S LOCATION ADDRESS ( IF DIFFERENT ) |
LOCATION # |
|||
A |
|
|
|
|
|
|
|
|
|
PHONE NUMBER |
EMPLOYER FEIN |
|
|
|
|
INDUSTRY CODE |
|
L |
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
C |
|
CARRIER ( NAME, ADDRESS & PHONE NO ) |
|
POLICY PERIOD |
CLAIMS ADMINISTRATOR ( NAME, ADDRESS & PHONE NO ) |
|||
A |
C |
|
|
TO |
|
|
|
|
|
|
|
|
|
|
|||
|
L |
|
|
|
|
|
|
|
RA I
R |
M |
|
|
|
|
|
|
|
CHECK IF APPROPRIATE |
|
|
|
|
|
|
|
|
|
|
|
|||||
S |
|
|
|
|
|
|
|
|
SELF INSURANCE |
|
|
|
|
|
|
|
|
|
|
|
|||||
I |
A |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
D |
CARRIER FEIN |
|
|
|
POLICY / |
|
|
|
|
ADMINISTRATOR FEIN |
|
|
|
|
||||||||||
E |
M |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
I |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
R |
N |
AGENT NAME & CODE NUMBER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
NAME ( LAST, FIRST, MIDDLE ) |
|
|
|
|
|
DATE OF BIRTH |
SOCIAL SECURITY NUMBER |
DATE HIRED |
|
|
|
STATE OF HIRE |
|||||||||||
E |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
M |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
ADDRESS ( INCL ZIP ) |
|
|
|
|
|
|
GENDER |
|
MARITAL STATUS |
OCCUPATION/JOB TITLE OR (SOC) |
||||||||||||||
P |
|
|
|
|
|
|
|
|
|
MALE |
|
|
UNMARRIED |
CODE |
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
L |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SINGLE/DIVORCED |
|
|
|
|
|
|
|
|
||
O |
|
|
|
|
|
|
|
|
|
FEMALE |
|
|
MARRIED |
EMPLOYMENT STATUS |
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Y |
|
|
|
|
|
|
|
|
|
UNKNOWN |
|
|
SEPARATED |
|
|
|
|
|
|
|
|
||||
E |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
E |
|
PHONE NUMBER |
|
|
|
|
|
|
# OF DEPENDENTS |
|
UNKNOWN |
NCCI CLASS CODE |
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
W |
|
RATE |
|
PER: |
|
DAY |
|
MONTH |
# DAYS WORKED/WEEK |
|
FULL PAY FOR DAY OF INJURY? |
|
YES |
|
NO |
||||||||||
A |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
G |
|
|
|
|
|
WEEK |
|
OTHER: |
|
|
|
|
|
|
DID SALARY CONTINUE? |
|
|
|
YES |
|
NO |
||||
E |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
TIME EMPLOYEE |
AM |
DATE OF INJURY/ILLNESS |
TIME OF |
|
|
AM |
LAST WORK |
|
DATE EMPLOYER |
DATE DISABILITY BEGAN |
|||||||||||||
|
|
BEGAN WORK |
|
|
|
|
OCCURRENC |
|
|
|
DATE |
|
NOTIFIED |
|
|
|
|
|
|
|
|
||||
|
|
|
PM |
|
|
|
E |
|
|
|
|
PM |
|
|
|
|
|
|
|
|
|
|
|
|
|
O |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
C |
|
CONTACT NAME / PHONE NUMBER |
|
|
|
|
|
TYPE OF INJURY/ILLNESS |
|
|
|
PART OF BODY AFFECTED |
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
C |
|
DID INJURY/ILLNESS EXPOSURE OCCUR ON EMPLOYER'S PREMISES? |
|
TYPE OF INJURY / ILLNESS CODE |
PART OF BODY AFFECTED CODE |
|
|
||||||||||||||||||
|
|
YES |
|
|
NO |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
U |
|
DEPARTMENT OR LOCATION WHERE ACCIDENT OR ILLNESS EXPOSURE |
|
|
ALL EQUIPMENT, MATERIALS, OR CHEMICALS EMPLOYEE WAS USING WHEN |
|
|
||||||||||||||||||
|
|
OCCURRED |
|
|
|
|
|
|
|
ACCIDENT OR ILLNESS EXPOSURE OCCURRED |
|
|
|
|
|
|
|
||||||||
R |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
|
|
SPECIFIC ACTIVITY THE EMPLOYEE WAS ENGAGED IN WHEN THE ACCIDENT OR |
WORK PROCESS THE EMPLOYEE WAS ENGAGED IN WHEN ACCIDENT OR ILLNESS |
||||||||||||||||||||||
R |
|
ILLNESS EXPOSURE OCCURRED |
|
|
|
|
|
|
EXPOSURE OCCURRED |
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
E
HOW INJURY OR ILLNESS / ABNORMAL HEALTH CONDITION OCCURRED. DESCRIBE THE SEQUENCE OF EVENTS AND INCLUDE ANY OBJECTS OR SUBSTANCES THAT DIRECTLY INJURED THE EMPLOYEE OR MADE THE EMPLOYEE ILL.
|
N |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CAUSE OF INJURY CODE |
|
||
|
C |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
E |
DATE RETURNED TO WORK |
IF FATAL, GIVE DATE OF DEATH |
WERE SAFEGUARDS OR SAFETY EQUIPMENT PROVIDED? |
|
|
YES |
|
NO |
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
WERE THEY USED? |
|
|
YES |
|
NO |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
T |
PHYSICIAN / HEALTH CARE PROVIDER ( NAME & ADDRESS ) |
|
|
HOSPITAL ( NAME & ADDRESS ) |
|
INITIAL TREATMENT |
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
R |
|
|
|
|
|
|
|
|
|
NO MEDICAL TREATMENT |
|
||
|
E |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
A |
|
|
|
|
|
|
|
|
|
MINOR: BY EMPLOYER |
|
||
|
T |
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
M |
|
|
|
|
|
|
|
|
|
MINOR CLINIC/HOSPITAL |
|
||
|
E |
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
N |
|
|
|
|
|
|
|
|
|
EMERGENCY CARE |
|
|
|
|
T |
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
O |
WITNESSES ( NAME & PHONE # ) |
|
|
|
|
|
|
|
HOSPITALIZED > 24 HRS |
|
|||
|
|
|
|
|
|
|
|
|
|
FUTURE MAJOR MEDICAL/ |
|
|||
|
T |
|
|
|
|
|
|
|
|
|
|
|||
|
H |
|
|
|
|
|
|
|
|
|
LOST TIME ANTICIPATED |
|
||
|
DATE ADMINISTRATOR NOTIFIED |
|
DATE PREPARED |
PREPARER'S NAME & TITLE |
|
|
|
|
|
|
||||
|
E |
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
R |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
NM WCA FORM E1.2 |
EQUIVALENT TO OSHA'S FORM 301 |
FORM |
|
|||||||||||
Completion of this form is not an admission that the claim is compensable under the Workers’ Compensation Act.
|
NEW MEXICO WORKERS' COMPENSATION ADMINISTRATION |
||
Phone: (505) |
|||
FARMINGTON: |
LAS CRUCES: |
||
LAS VEGAS: |
LOVINGTON: |
||
Roswell: |
Santa Fe: |
||
FILING INSTRUCTIONS
PURPOSE: To report all alleged
completed by the employer or the employer's representative.
WHEN TO FILE: This form must be filed within 10 days of knowledge of any alleged
WHERE TO FILE: Mail the original form to the New Mexico Workers' Compensation Administration (Attention: Statistics) at the address on the front of this form. Copies must also be provided to the worker and the employer's workers' compensation insurer.
PENALTIES: Each instance of failure to file this form when required is punishable by a fine of up to $1,000.00.
INSTRUCTIONS FOR COMPLETION
FILLING IN THE SHADED AREAS IS OPTIONAL. The employer may wish, however, to use some of these areas (such as "Witnesses") for the employer's records. Expanded instructions are found in the publication Guide to Completing the Employer's First Report of Injury or Illness, available from the Administration's Albuquerque office (call either number
Please print in black ink or type, and ensure that all entries are legible before submission. An illegible or incomplete E1 may be returned.
NAIC CODE: Represents the nature of the employer's business at the location where the worker was employed at the time of injury or illness exposure; derived from the federal government publication North American Industry Classification System Manual. Include this code if known.
EMPLOYER'S LOCATION ADDRESS: Facility where the worker was employed at the time of injury, if different from mailing address.
CARRIER: Name, mailing address and telephone number of the licensed business entity issuing a contract of insurance and assuming financial responsibility on behalf of the employer. A
CLAIMS ADMINISTRATOR: Name, mailing address and telephone number of the insurance carrier, agency, third party administrator or
EMPLOYER, CARRIER OR ADMINISTRATOR FEIN: Federal Identification Number, assigned by the Internal Revenue Service.
DID SALARY CONTINUE? Shows if the employer is continuing to pay the worker's regular wages without charge to employee benefits.
DATE OF INJURY/ILLNESS: In the case of an occupational illness (arising from the worker's activity or exposure over an extended period), enter the date of diagnosis or the date first reported to the employer as possibly
DATE EMPLOYER NOTIFIED: The date the worker first notified (verbally or in writing) the employer or the employer's representative of the alleged
DATE DISABILITY BEGAN: The first full day on which the worker lost time from work due to the injury or illness.
TYPE OF INJURY OR ILLNESS: Briefly describe the nature of the injury (such as lacerations to the forearm) or illness (such as carpal tunnel syndrome). Be as specific as possible.
PART OF BODY AFFECTED: The specific part of body affected by the injury or illness (for example, right forearm, lower back).
DEPARTMENT OR LOCATION: If the accident or illness exposure did not occur on the employer's premises, enter specific address or location (for example, Client's office at 123 Main St., Yourtown, NM 87xxx). For occurrences in New Mexico, give ZIP or COUNTY.
ALL EQUIPMENT, MATERIAL OR CHEMICALS: List all equipment, materials and/or chemicals the worker was using, applying, handling or operating when the injury or illness exposure occurred. Be specific (for example, decorator's scaffolding, electric sander, paintbrush and paint). Enter "NA" if not applicable. NOTE: The items listed do not have to be directly involved in the worker's injury or illness.
SPECIFIC ACTIVITY: Describe the specific activity the worker was engaged in when the accident or illness exposure occurred (for example, sanding ceiling woodwork in preparation for painting).
WORK PROCESS: Describe the work process the worker was engaged in when the accident or exposure occurred, such as building maintenance. Enter "NA" for not applicable if not engaged in a work process (for example, if the worker was walking along a hallway).
HOW INJURY OR ILLNESS OCCURRED: Describe how the injury or illness/abnormal health condition occurred. Be very specific. Include the sequence of events and name any objects or substances that directly injured the worker or made the worker ill. (For example: worker stepped back to inspect work and slipped on some scrap metal. As worker fell, worker brushed against the hot metal.)
WORKER'S/EMPLOYER'S RIGHTS AND RESPONSIBILITIES
If you, the worker, believe that benefits are due you under the Workers' Compensation Act, and your employer or the employer's insurance carrier has failed or refused to make those benefits available to you, you have a right to file a complaint with the New Mexico Workers' Compensation Administration. Workers and employers with questions about rights or responsibilities under the Act may contact an ombudsman at any Workers' Compensation Administration regional office for information and assistance. To do so, call any of the
Document Properties
| Fact | Detail |
|---|---|
| Purpose | To report alleged work-related injuries or illnesses resulting in more than 7 days of lost work or in death. |
| Filing Deadline | Within 10 days of knowledge of the alleged work-related injury or illness. |
| Location for Filing | Mail the original form to the New Mexico Workers' Compensation Administration at the address provided on the form. |
| Penalties for Non-Compliance | Failing to file the form when required can result in a fine of up to $1,000.00. |
| Governing Law(s) | Administered under the New Mexico Workers' Compensation Act. |
Steps to Filling Out New Mexico Report
After an employee reports a work-related injury or illness, their employer has a responsibility to fill out the New Mexico Workers' Compensation Administration's Employer's First Report of Injury or Illness form. This document is crucial for ensuring that the incident is officially recorded and that the employee can receive any necessary workers' compensation benefits. This process might seem daunting, especially during stressful times, but understanding and completing the form accurately is essential. The following steps will guide you through filling out the form.
- Write the employer's name and address, including the zip code, in the designated box at the top of the form.
- Enter the carrier/administrator claim number and OSHA log number, if applicable.
- Select the Report Purpose Code that best describes why you are filing this report.
- Fill in the Jurisdiction claim number and the insured report number as directed.
- If the employee’s work location address is different from the employer’s main address, provide it along with the location number.
- Include the employer's phone number and Federal Employer Identification Number (FEIN).
- Specify the industry code that represents the nature of the business.
- Provide the name, address, and phone number of the insurance carrier, policy period details, and the claims administrator’s information.
- If self-insurance is applicable, check the appropriate box and provide the Carrier FEIN, Policy/Self-Insured Number, and Administrator FEIN.
- Include the agent name and code number if known.
- Fill out the employee’s personal and employment information, including name, date of birth, social security number, date hired, state of hire, address, gender, marital status, occupation/job title or SOC code, employment status, phone number, and number of dependents.
- Specify the NCCI class code, rate per (day, month, week, or other), number of days worked per week, and whether full pay was given for the day of injury and if the salary continued.
- Record the date and time of the injury/illness, last work date before the injury/illness, date employer was notified, date disability began, and the date returned to work if applicable.
- Describe the type of injury/illness, part of the body affected, whether the injury/illness exposure occurred on the employer’s premises, and input the corresponding codes.
- Provide details about the department or location where the accident or illness exposure happened, including all equipment, materials, or chemicals the employee was using when the accident or illness exposure occurred.
- Explain the specific activity and work process the employee was engaged in when the accident or illness exposure occurred.
- Describe how the injury or illness/abnormal health condition occurred, including the sequence of events and any objects or substances that directly injured the employee or made the employee ill.
- If applicable, specify cause of injury code, if fatal, the date of death, and address safeguard or safety equipment-related questions.
- Provide information about the initial treatment provider and any witnesses.
- Fill in the date the administrator was notified, the date the form was prepared, and preparer’s name and title.
Once the form is completed, ensure all information is clear and legible. It should be filed within 10 days of knowledge of the employee's alleged work-related injury or illness. Remember, this form needs to be sent to the New Mexico Workers' Compensation Administration at the address provided at the top of the form and copies must be given to the worker and the employer's workers' compensation insurer. Completing this form accurately and promptly helps to ensure that the employee’s needs are addressed according to the Workers' Compensation Act.
Frequently Asked Questions
What is the purpose of the New Mexico Employers' First Report of Injury or Illness form?
This form is designed for employers to report any alleged work-related injuries or illnesses that result in more than seven days of lost work, or in the death of a worker. It's important to understand that completing and submitting this form is neither an admission of liability by the employer nor a denial that the injury or illness is work-related. It's a required step in making sure an incident is officially documented.
When must the New Mexico Employers' First Report of Injury or Illness form be filed?
Employers must ensure that this form is filled out and filed within ten days of becoming aware of any work-related injury or illness that causes the worker to lose more than seven days of work. This requirement to file is in place even if there is a dispute regarding the worker's claim of a work-related injury or illness.
Where should the Employers' First Report of Injury or Illness form be sent?
The original form needs to be mailed to the New Mexico Workers' Compensation Administration, specifically to the Statistics department at the address provided on the front of the form. Additionally, copies of this completed form must also be distributed to the injured or ill worker and to the employer's workers' compensation insurer, ensuring that all parties are properly informed.
Are there any penalties for failing to file the Report form on time?
Yes, employers face financial penalties if they fail to file the report as required. Specifically, each instance of failing to submit the form when required can result in a fine of up to $1,000. This underscores the importance of adhering to filing deadlines to avoid unnecessary costs.
What should be included when describing the type of injury or illness and how it occurred?
The description of the injury or illness should be specific and include details such as the nature of the injury (like lacerations to the forearm) or illness (such as carpal tunnel syndrome). Additionally, when explaining how the injury or illness occurred, include a clear sequence of events and identify any objects or substances that directly caused harm or illness to the employee. This might look like describing an employee stepping back, slipping on some scrap metal, and then coming into contact with hot metal as they fell. Accuracy and specificity are crucial in this section to provide a clear understanding of the circumstances surrounding the injury or illness.
Common mistakes
Filling out the New Mexico Report Form accurately is crucial for ensuring that workers' compensation claims are processed efficiently and effectively. However, mistakes can happen. Here are five common errors people make when completing this form:
Not using black ink or typing: The form specifically instructs to print in black ink or type. This requirement helps ensure that the information is legible and can be processed without delays. Using other colors or handwriting that is difficult to read can lead to processing errors or returned forms.
Omitting the NAICS code: While the form mentions that filling in the shaded areas is optional, including the NAICS (North American Industry Classification System) code can provide valuable context about the nature of the employer's business, which can be relevant in assessing the claim.
Failure to specify if salary continues: The section "Did salary continue?" is crucial for determining how compensation is handled. Not clarifying whether the worker's regular wages are being paid can cause unnecessary confusion and delays in the processing of benefits.
Leaving the description of the injury or illness vague: The form requires a specific description of the type of injury or illness and the part of body affected. General or vague descriptions can hinder the accurate processing of the claim, as the extent and nature of the injury or illness play a significant role in the evaluation process.
Not reporting the date the employer was notified: This date is pivotal because it triggers the countdown for certain reporting and filing obligations under the Workers' Compensation Act. Failure to accurately report this date can affect the timeliness and legality of the claim process.
Ensuring these details are accurately reported not only helps in the smooth processing of claims but also secures the rights and benefits for employees suffering from workplace injuries or illnesses. Always double-check the form before submission for a more straightforward and efficient claims process.
Documents used along the form
When managing workers' compensation claims in New Mexico, several key forms and documents are commonly used alongside the New Mexico Employers’ First Report of Injury or Illness form. These documents play crucial roles in the claims process, ensuring proper communication, compliance, and facilitation of benefits for injured workers. It's vital for employers, insurance carriers, and claims administrators to be familiar with each document's purpose and requirements.
- WCA Form E1.3 - Wage and Supplemental Benefits Report: This form is critical for determining the injured worker's compensation rate. It provides detailed information about the worker's earnings, enabling the calculation of wage replacement benefits.
- Notice of Accident Form: Workers must use this form to officially notify their employer of a work-related injury or illness. Timely submission is essential for preserving the right to claim workers' compensation benefits.
- Employer’s Report of Occupational Injury or Illness to OSHA (Form 300): Employers are required to maintain records of work-related injuries and illnesses. This OSHA form is part of a larger requirement to document and report workplace injuries and illnesses for safety monitoring and improvements.
- WCA Form C - Certificate of Insurance Coverage: This document verifies that the employer has the necessary workers' compensation insurance coverage. It is important for proving compliance with state laws mandating coverage for employees.
- Proof of Compliance Form: Employers must submit this form to the New Mexico Workers' Compensation Administration to demonstrate adherence to state regulations regarding workers' compensation insurance.
- Medical Release Form: This form authorizes the release of the injured worker's medical records to the employer or insurance carrier. It is crucial for assessing the nature and extent of the injury or illness and facilitating appropriate medical treatment.
These documents complement the New Mexico Employers' First Report of Injury or Illness by providing deeper context, substantiating claims, and aiding in the efficient processing and management of workers' compensation cases. Familiarity with these forms ensures that all parties involved in the workers' compensation process can navigate it effectively, upholding the rights and responsibilities prescribed by law.
Similar forms
The New Mexico Report form is similar to several other documents used in various regulatory and administrative settings, providing a structured way to report specific details. One such document is the Federal Occupational Safety and Health Administration's (OSHA) Form 301, Injury and Illness Incident Report. Like the New Mexico Report form, the OSHA Form 301 gathers detailed information about work-related injuries and illnesses, focusing on specifics such as the injured or ill employee's name, the date and time of the event, and a description of the injury or illness. Both forms serve a crucial role in documenting incidents to help improve workplace safety and health. Yet, the New Mexico form stands apart by including data points tailored to the state's requirements, such as jurisdiction claim number and New Mexico Workers' Compensation Administration (NMWCA) contact information.
Another document resembling the New Mexico Report form is the First Report of Injury or Illness form used in other states, often referred to by designations such as 'DWC-1' in jurisdictions like California. Although these forms are customized to meet the specific regulatory and data requirements of their respective states, they share a common goal: to capture essential information about workplace incidents that result in injury or illness. The shared elements between the New Mexico form and others like DWC-1 include employer and insurance carrier information, details of the injury or illness (including type, cause, and body part affected), and treatment information. However, nuances in state laws and the specifics of workers' compensation systems necessitate slight variations in the information each form collects. The emphasis is consistently on clear, concise, and complete reporting to facilitate the claims process and contribute to ongoing efforts to make workplaces safer.
Dos and Don'ts
When completing the New Mexico Workers' Compensation Administration Employers' First Report of Injury or Illness, attention to detail and accuracy is paramount. Below are guidelines on what should and shouldn't be done during the form filling process.
Things You Should Do:- Use Black Ink or Type: It's important to ensure that all entries are legible. The instructions specifically mandate printing in black ink or typing, which helps in avoiding errors and ensures clarity for all parties involved.
- Provide Detailed Descriptions: When describing the injury or illness, and how it occurred, be as specific as possible. Detailed descriptions will help in the assessment of the report and in decision-making processes related to the claim.
- Report Timely: The form needs to be filed within 10 days of knowledge of any work-related injury or illness that results in more than 7 days of lost work. Timeliness in filing is not just a matter of compliance but can significantly affect the processing of the claim.
- Complete All Required Sections: Make sure all necessary sections of the form are filled out. Even though some areas are marked optional, providing comprehensive information can facilitate the claim's processing and avoid unnecessary delays.
- Omit Contact Information: Failing to provide complete contact information for the employer, carrier, or claims administrator can lead to delays. Contact information is crucial for follow-up and clarification.
- Leave Questions Unanswered: If you encounter a question that you believe doesn’t apply, it’s better to mark it as "Not Applicable" (NA) instead of leaving it blank. This demonstrates that you acknowledged all parts of the form.
- Provide Incomplete Descriptions: Avoid vague descriptions of the injury, illness, or incident. Incomplete descriptions can lead to misunderstandings about the nature and severity of the injury or illness.
- Ignore Submission Guidelines: Do not disregard the filing instructions, including where to file and providing copies to the worker and the employer's workers' compensation insurer. Incorrect filing can result in the form being returned or not processed timely.
Adhering to these guidelines ensures that the process of reporting an injury or illness complies with the New Mexico Workers' Compensation Administration's requirements and helps in the efficient handling of the workers' compensation claim.
Misconceptions
Many people hold misconceptions about the New Mexico Report form, which can lead to confusion and errors in completing and submitting this important document. Below, we address some of these misunderstandings to help clarify the process.
- Misconception 1: The form is an admission of liability by the employer. This is incorrect. Completing and submitting the form is not an admission that the claim is compensable under the Workers' Compensation Act. It is merely a report of an injury or illness.
- Misconception 2: All sections of the form must be filled out. Not all shaded areas are mandatory. While it is crucial to provide as much detail as possible, some sections are optional and for the employer's records, such as the "Witnesses" section.
- Misconception 3: The form should only be filed for severe injuries. Actually, the form must be filed within 10 days of knowledge of any alleged work-related injury or illness that results in more than 7 days of lost work, regardless of the perceived severity.
- Misconception 4: Only the original form is required. The employer must mail the original form to the Workers' Compensation Administration and also provide copies to the injured worker and the employer's workers' compensation insurer.
- Misconception 5: There are no penalties for not filing the form. Employers who fail to file this report as required are subject to a fine of up to $1,000.00 for each instance of non-compliance.
- Misconception 6: The form doesn't need to be legible. An illegible or incomplete form may be returned. It is essential that all entries are legible and the form is filled out completely to ensure accurate processing.
Understanding these aspects of the New Mexico Report form is vital for employers to navigate the workers' compensation claim process effectively and comply with the state's regulations. It streamlines the process for all parties and ensures that injured workers receive the attention and support they need.
Key takeaways
The New Mexico Report form is a vital document for reporting work-related injuries or illnesses under the jurisdiction of the state's Workers' Compensation Administration. Understanding the key elements about filling out and utilizing this form can ensure compliance and safeguard the rights and responsibilities of both employers and employees. Here are eight key takeaways:
- The form must be used by employers to report any alleged work-related injuries or illnesses that result in more than seven days of lost work or in the death of a worker. It serves as neither an admission nor a denial of the claim's compensability.
- Employers are required to fill the form out and submit it within 10 days of becoming aware of any alleged work-related injury or illness meeting the above criteria.
- The original form should be mailed to the New Mexico Workers' Compensation Administration at the provided address, with copies also being provided to the affected worker and the employer's workers' compensation insurer.
- Failure to file this form as required can lead to fines up to $1,000.00 per instance of non-compliance, emphasizing the legal obligation tied to this documentation.
- When completing the form, it's important to use black ink or type to ensure all entries are legible. Incomplete or illegible forms may be returned, potentially delaying the processing of claims.
- Some sections of the form, particularly those in shaded areas, are optional and meant for the employer's records, such as the "Witnesses" section. However, providing complete and detailed information can aid in the claim's evaluation process.
- The section on how the injury or illness occurred demands detailed documentation, requiring a description of the sequence of events and any objects or substances that directly contributed. Accurate and thorough details are crucial for a clear understanding of the circumstances surrounding the incident.
- Workers who believe they are entitled to benefits under the Workers' Compensation Act and face difficulties in receiving them from their employer or the employer's insurance carrier have the right to file a complaint with the New Mexico Workers' Compensation Administration. Assistance from an ombudsman is available at any of the Administration's regional offices.
Filling out the New Mexico Report form accurately and comprehensively plays a pivotal role in the workers' compensation process, ensuring that workers' rights are protected while meeting the statutory requirements set by the state. Employers should familiarize themselves with the form and its requirements to maintain compliance and support their employees effectively in the event of a workplace injury or illness.
Common PDF Templates
New Mexico Courts - Ensures that the plaintiff's demands, whether financial compensation or recovery of property, are clearly defined from the outset of the legal proceedings.
Land Contract Template - A clause detailing the process and obligations for transferring possession of the property post-closing emphasizes clarity and fairness in terms of occupancy.
Rpd-41367 - Empowers owners to verify and reconcile tax withholdings against their calculated tax responsibilities.